|
Proteinuria Predicts Good Renal Results in Lupus Nephritis - Renal and Urology News |
 |
 |
May 08, 2015

Uric acid levels affect kidneys
(HealthDay News) -- Proteinuria levels at 12 months are the best predictor of long-term renal outcome in patients with lupus nephritis, according to a study published in the May issue of Arthritis & Rheumatology.
Maria Dall'Era, M.D., from the University of California in San Francisco, and colleagues analyzed data from the Euro-Lupus Nephritis Trial to evaluate the performance of proteinuria, serum creatinine (Cr), and urinary red blood cells (RBCs) as predictors of good long-term renal outcome (defined as a serum Cr value ?1.0 mg/dL) in patients with lupus nephritis. 76 patients were followed for a minimum of 7 years.
The researchers found that a proteinuria value of <0.8 gm/day at 12 months after randomization was the single best predictor of good long-term renal function (sensitivity of 81% and specificity of 78%). The performance of the outcome measure was not improved with the addition of serum Cr to proteinuria. Sensitivity dropped to 47% with the addition of urinary RBCs.
The authors suggest "that urinary RBCs should not be included as a component of clinical trial response criteria in lupus nephritis."
One author disclosed financial ties to the pharmaceutical industry.
Source
- Dall'Era, M, et al. Arthritis & Rheumatology; doi: 10.1002/art.39026.
|
|
Advances in immunotherapy for renal cell carcinoma - ScienceBlog.com (blog) |
|
|
|
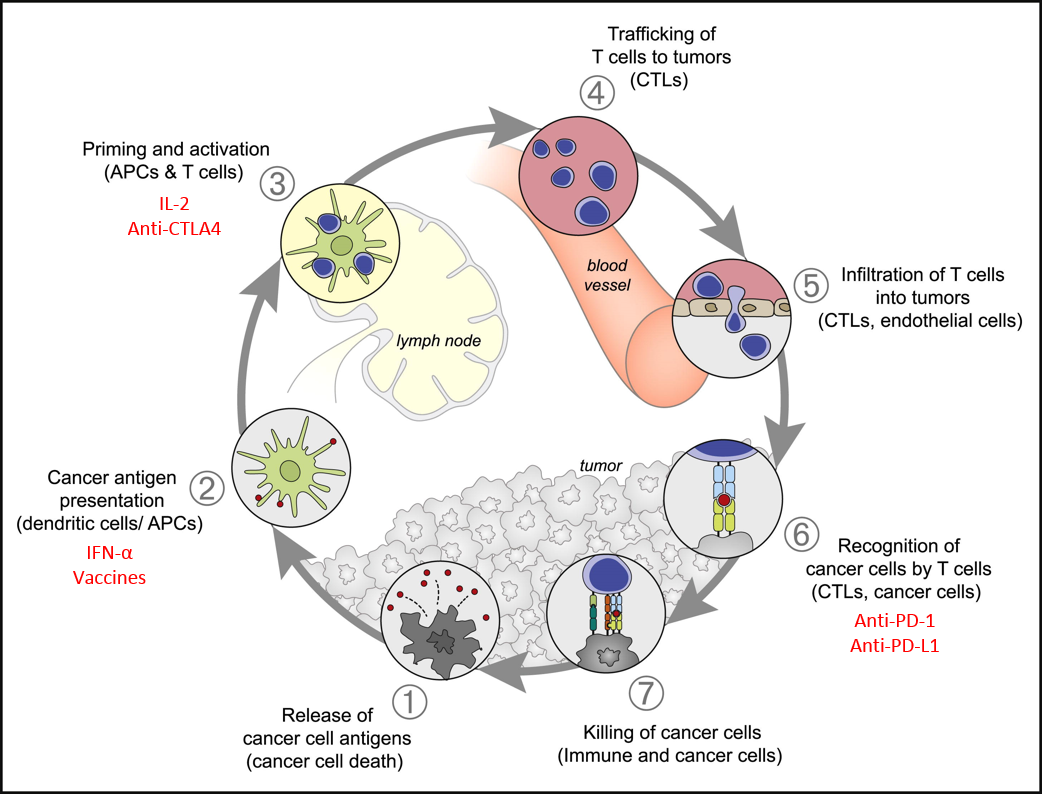
In recent years there has been renewed interest in immunotherapies to treat of metastatic renal cell carcinoma (mRCC). Immunotherapies increase the body’s natural finely regulated multiple-step anti-tumour immune response (Figure 1). The balance of stimulatory and inhibitory signals (reviewed in Chen & Mellman, 2013) are important in maintaining self-tolerance and modulating normal immune responses to minimising health tissue damage. However, tumours can develop mechanisms to evade this immune response.
Figure 1: Immune Response Cycle. The major steps in the immune response cycle to cancer cells. Immunotherapies target a number of different steps (red). Modified from Chen & Mellman (2013) Immunity 39, 1-10.
The approved immunotherapies for RCC are the cytokines Interferon-alpha (IFN-?) and Interleukin-2 (IL-2) to stimulate T-cell activity. Unfortunately this can result in a variety of treatment related toxicities. The response rate to these drugs is relatively low but the responses are more likely to be durable. An alternative strategy is to inhibit specific immune checkpoints that normally act to limit excessive immune activity. The numerous stimulatory and inhibitory checkpoints in the immune system minimise the death of healthy, “self” cells in an immune response. The presence of inhibitory signals on tumour cells can therefore stop an immune response but the blockade of these inhibitory signals can increase the immune response and tumour cell death. A list of ongoing trials is available here.
One such inhibitor is Cytotoxic T-Lymphocyte Antigen 4 (CTLA-4) which when bound to B7-1 or B7-2 disrupts early T-cell activation and blocks cytokine production. Ipilumumab binds to CTLA-4 and blocks this inhibition resulting in increased production of auto-reactive T-cells and cytokines. While some patients have responded well to ipilumumab there are some severe adverse events (AE) associated with off-target effects of this drug (Yang et al., 2007).
A different checkpoint target is the Programmed cell Death-1 (PD-1)/PD-L1 inhibitory signalling pathway which reduces T-cell signalling and activation helping to maintain peripheral tolerance. Anti-PD-1 antibodies – nivolumab, pembrolizumab and pidilizumab – and the anti-PD-L1 antibody MPDL3280A are effective at blocking this signalling. PD-1 is expressed on a range of immune cells and PD-L1 can be expressed by tumour cells minimising the immune response. Nivolumab is the most frequently used anti-PD-1 in RCC and early phase trials have shown enhanced long-term survival (Lipson et al., 2013), with varied doses of nivolumab inducing comparable response rates with manageable toxicity profiles (Motzer et al.,2015). There are also numerous ongoing trials investigating pembrolizumab which showed some response in melanoma patients but can have severe AE (Martin-Liberal et al., 2015).
An alternative, and potentially complimentary, approach would be the use of cancer vaccines to prime the immune system for response to cancer cells. The introduction of antigen presenting cells (APCs) loaded with tumour-derived RNA, such as AGS-003, induces a tumour-specific immune response (Amin et al., 2015). A synthetic vaccine, IMA901, consists of 10 Tumour Associated Peptides (TUMAPs) bound to HLA ligands for presentation to the immune system and as in early trials (Bedke & Stenzl, 2013).
The immune related AEs (irAE) seen in immunotherapy drug trials can differ from AE from other drug types and can be severe (Weber et al., 2012). Early diagnosis and effective toxicity management is required to ensure ongoing treatment is tolerable. Early trials suggest a correlation between response rate and frequency of irAEs and perhaps such irAEs could be worth enhanced survival. Further trials will also determine any risk of sequential toxicities that could impact on treatment regimens.
In addition to the development of therapies there is also a great need for research into relevant biomarkers; currently there are only indicative and not predictive biomarkers to determine which patients are most likely to response. Patient selection could also reduce the use of ineffective treatments which have a high irAE risk but no or minimal health benefit. Patient fitness and toxic burden also needs to be considered as frailer patients may not be able to tolerate AEs or to survive an initial decline before response begins.
As immunotherapies develop they may also be beneficial as adjuvant treatments following surgical resection. The responses to immunotherapies can be durable, continuing long after treatment has completed indicating the formation of tumour specific immune memory; they could therefore also be useful in reducing recurrence risk in high risk patients such as those with hereditary forms of RCC.
- Amin A, Dudek AZ, Logan TF, Lance RS, Holzbeierlein JM, Knox JJ, Master VA, Pal SK, Miller WH Jr, Karsh LI, Tcherepanova IY, DeBenedette MA, Williams WL, Plessinger DC, Nicolette CA, Figlin RA (2015). Survival with AGS-003, an autologous dendritic cell-based immunotherapy, in combination with sunitinib in unfavorable risk patients with advanced renal cell carcinoma (RCC): Phase 2 study results. J Immunother Cancer Apr 21;3:14. PMID: 25901286.
- Bedke J, Stenzl A (2013) IMA901: a peptide vaccine in renal cell carcinoma. Expert Opin Investig Drugs Oct;22(10):1329-36. Review. PMID: 23899354.
- Chen DS, & Mellman I (2013). Oncology meets immunology: the cancer-immunity cycle. Immunity, 39 (1), 1-10 PMID: 23890059.
- Lipson EJ, Sharfman WH, Drake CG, Wollner I, Taube JM, Anders RA, Xu H, Yao S, Pons A, Chen L, Pardoll DM, Brahmer JR, Topalian SL (2013). Durable cancer regression off-treatment and effective reinduction therapy with an anti-PD-1 antibody. Clin Cancer Res Jan 15;19(2):462-8. PMID: 23169436.
- Martin-Liberal J, Kordbacheh T, Larkin J (2015). Safety of pembrolizumab for the treatment of melanoma. Expert Opin Drug Saf Apr 30:1-8. [Epub ahead of print] PMID: 25927979.
- Motzer RJ, Rini BI, McDermott DF, Redman BG, Kuzel TM, Harrison MR, Vaishampayan UN, Drabkin HA, George S, Logan TF, Margolin KA, Plimack ER, Lambert AM, Waxman IM, Hammers HJ (2015). Nivolumab for Metastatic Renal Cell Carcinoma: Results of a Randomized Phase II Trial. J Clin Oncol May 1;33(13):1430-7. PMID: 25452452.
- Weber JS, Kähler KC, Hauschild A (2012). Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol Jul 20;30(21):2691-7. PMID: 22614989
- Yang JC, Hughes M, Kammula U, Royal R, Sherry RM, Topalian SL, Suri KB, Levy C, Allen T, Mavroukakis S, Lowy I, White DE, Rosenberg SA (2007). Ipilimumab (anti-CTLA4 antibody) causes regression of metastatic renal cell cancer associated with enteritis and hypophysitis. J Immunother Nov-Dec;30(8):825-30. PMID: 18049334.
|
|
|
Blood Pressure Variability Among Chronic Dialysis Patients - Medscape |
|
|
|
 Blood Pressure Variability Among Chronic Dialysis Patients Blood Pressure Variability Among Chronic Dialysis Patients
Medscape
A growing body of evidence suggests that both short-term and long-term BPV are associated with adverse events among chronic dialysis patients. Over the last 18 months, several studies have linked long-term BPV (considered dialysis treatment to dialysis ...
|
|
|
Dialysis dilemma brings new option for rural Alabama residents - WTVM |
|
|
|
PERRY CO., AL (WSFA) -
How would you choose to spend four hours of your day? For more than 8,000 people in Alabama, that time is a matter of life or death. Many spend it on a dialysis machine -- the only way they can eliminate waste and unwanted water from their blood.
Despite the critical nature, some patients would rather forgo treatment than travel to a clinic. That is, until the state stepped in.
For at least three hours a day, three days a week, Henry Kelly gets hooked up to a dialysis machine for treatment. He uses the time in the chair to think about why it's important for him to be here.
"My mom, my brother were all on dialysis," Kelly recalls, "and they passed away on dialysis."
High blood pressure issues led him to dialysis treatment, a chronic illness that affected his brother and mother before their deaths. Kelly's mother also suffered from diabetes. He says she died following one of many long trips home from treatment.
His mother didn't live to see the Davita Center open in 2013. It serves 32 people in four different counties. More importantly, it's only minutes away from residents who need it.
Before the Davita Center was built, rural Perry County dialysis patients had two options for treatment: Drive the 30 minutes to Selma in Dallas County or double the distance to about 55 minutes by going to Demopolis in Marengo County. When factoring in the round trip, the time for treatment was simply too overwhelming for some patients.
"You had people choosing not to go to dialysis, and when that happens you die." explained Ron Sparks, appointed Director of the Black Belt Commission by Governor Robert Bentley. He learned early of the lack of health care options in rural counties.
"The lack of health care in these rural areas is a serious problem," Sparks says, "especially when it comes to dialysis."
Francis Ford set out to change that. She's a retired nurse and the health care coordinator in Perry County. A woman determined to stop the dying. "We didn't just only write letters ourselves, but we got patients to write, we got local citizens to write in the community. We had the support of our commissioners..."
And, she found the support of the governor. Bob Riley was in office at the time, and Chad Nichols was then head of the Black Belt Commission. He had a personal interest. His grandfather was a dialysis patient who lived in Perry County. He traveled to Selma for treatment.
"Going to dialysis, he was in a major car accident," Nichols remembered. "So I saw the impact it had on him..."
The first hurdle for Nichols and Ford was getting rid of a 1975 state health regulation that required a hospital within 25 miles of a dialysis center. Back in '75 there were 128 hospitals in Alabama. Today, there are just 92 and at least 10 have closed in the past 3 years .
"Shocked," Nichols reacted, "but also sadden that a state regulation was on the books that was, in my view, really impacting the quality of life and impacting or making life and death decisions at a time for people who didn't have the ability to travel to get care."
The state health department eliminated the rule back in 2005. More than 10 years and two governors later, Perry County finally has its own dialysis center.
"I don't think many people realize if you have not walked in the shoes of a person on dialysis, you don't know the hardship it is and the burden it is on that person's family," Ford expressed.
Henry Kelly no longer travels to Selma for treatment. He now comes to the Davita Center not far from where he lives. It means less time on the road and more time to think about life beyond the chair.
With the rule change, more centers can open in rural counties. But those areas usually run into other problems like health care costs. Since an overwhelming number of dialysis patients living in rural counties depend on public assistance, the reimbursement rate for the center is low. That means it's difficult for companies to make a profit.
If you have high blood pressure or diabetes you could be at risk for becoming a dialysis patient.
CLICK HERE to visit the Alabama Kidney Foundation where you can find risk factors that could help save your life.
Copyright 2015 WSFA 12 News. All rights reserved.
|
|
 Log in to explore the world's most comprehensive database of dialysis centres for free!
Log in to explore the world's most comprehensive database of dialysis centres for free!